We are republishing an open letter published this day, with the kind permission of its author.
To the attention of:
Dr. Vic Arendt
Dr. Claude Muller
Dr. Gérard Schockmel
Dr. Thérèse Staub
Dr. Paul Wilmes
Copy:
Prime Minister of Luxembourg
Luxembourg, 17/1/2022
Dear scientific and health experts,
I was surprised to read in the press your conclusions, which in the light of current scientific and medical literature appear entirely unjustified.
For these reasons I decided to challenge your conclusions as questioning is a common scientific practice.
I hope that the two first experts, found having produced five (5) and one (1) scientific publications respectively in their domains within the recent 10 years, might be accustomed in questioning and data analysis and not tending to expect unconditional acceptance.
What is a vaccine
Until the invention of the covid19 vaccine market, previous vaccines were based in a harmless-made virus which combined with adjuvants would trigger an immune response.
Since the SARS-Cov-2 virus has NOT until today been isolated, it certainly therefore remains impossible to continue with previous approach. This is also the reason for all failed previous coronavirus vaccine attempts in animals.
The method applied by current DNA and mRNA vendors needs to manipulate the human immune system to achieve the protection sought. This method rather belongs to the category of gene and cell therapy (a business domain of European Commission’s president’s husband). It was very well pointed out recently by a Bayer executive in a conference, that public would have never ever accept the gene therapy injections, so the term vaccine was a successful marketing application as far as it concerns customers.
Besides, these experimental pharmaceutical products do not act as vaccines, in what amounts to stopping transmission and infection, as mass data coming from UK and Israel have demonstrated.
We therefore must admit dealing with THERAPIES consisting of repeated injections, as Pfizer’s intentions clearly target multiple “booster” shots.
Efficacy and safety
Initial data of Pfizer/BioNtech
The initial Pfizer summary data submitted to FDA for approval were found unconvincing, as the article in BMJ explained,https://blogs.bmj.com/bmj/2020/11/26/peter-doshi-pfizer-and-modernas-95 -vaccins-efficaces-soyons-prudents-et-prenons-en-première-toutes-les-données/
Needless to say, that I went and cross-checked the claims of Dr. P. Doshi straight inside the Pfizer document.
A particularly dark point of this initial submission is the non-disclosure of the absolute risk reduction (ARR) for this product. In fact, despite long standing obligation of the pharma companies to calculate and publicize the ARR, Pfizer, at the discretion of FDA omitted this important parameter of the so-called gold standard of the FDA. You may examine the publication https://doi.org/10.3390/medicina57030199 o discover that the absolute efficacy of the Pfizer product is as low as of 0.7%; 95% CI, 0.59% to 0.83%; p < 0.000, and this already in November 2020.
Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine https://www.nejm.org/doi/full/10.1056/nejmoa2034577
FDA Briefing Document, Dec 10, 2020 https://www.fda.gov/media/144245/download
In case you may wonder about the credentials of Dr. P. Doshi, I prefer pointing out among others he was the brave scientist to bring down the recent STATIN fraud.
The troubles with this company go on as far as it concerns the trial design that is unfit for covid-19 reality and safety controls:
- Animal testing was skipped
- Phases II/III were combined
- After 2 months of Phase II/III, Emergency Use Authorized
- The trials were unblinded
- Phase III trials are ongoing until 2023
The demographics were misleading and had the wrong target population (only 4% of age 75+ contrary to the fact that 58% of high-risk people are over 75 years old).
The comorbidities also were unrepresented: 95% of people who have died with COVID-19 have had at least 1 co-morbidity listed as cause of death. The average is 4 comorbidities.
Subsequent data of Pfizer/BioNtech
The 6-months Pfizer’s follow-up report of below (its appendix), authored by scientists on the Pfizer payroll (only 16% without financial relationship) raises serious questions regarding cardiac safety signals.
Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months https://www.nejm.org/doi/full/10.1056/NEJMoa2110345
The 6 Month Supplementary Appendix https://www.nejm.org/doi/suppl/10.1056/NEJMoa2110345/suppl_file/nejmoa2110345_appendix.pdf
A significant safety report is also authored below.
US COVID-19 Vaccines Proven to Cause More Harm than Good Based on Pivotal Clinical Trial Data Analyzed Using the Proper Scientific Endpoint, “All Cause Severe Morbidity”https://www.scivisionpub.com/abstract-display.php?id=1811
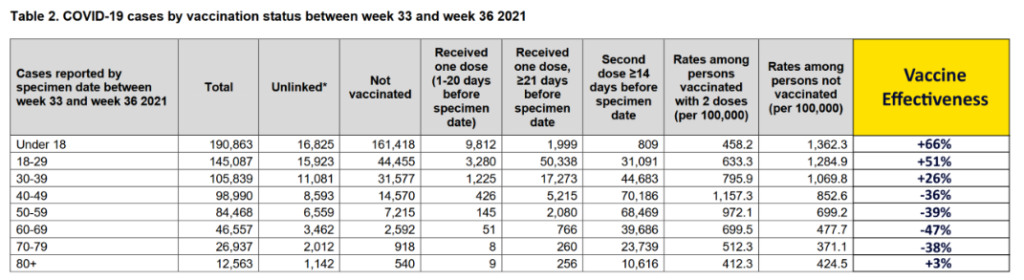
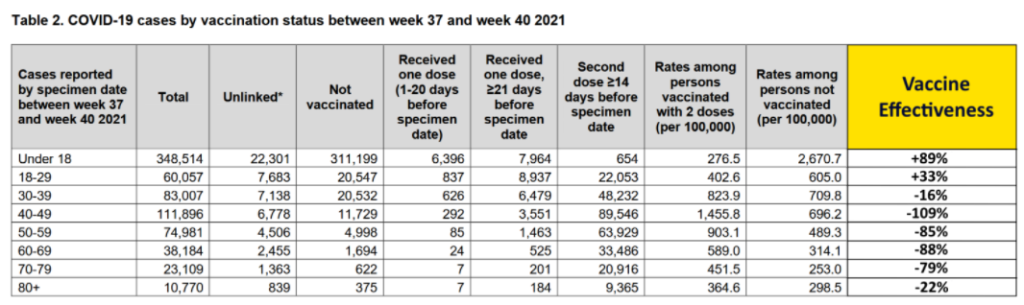
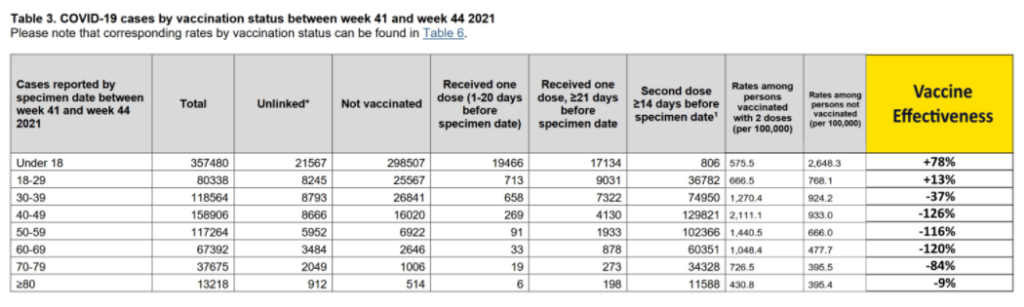
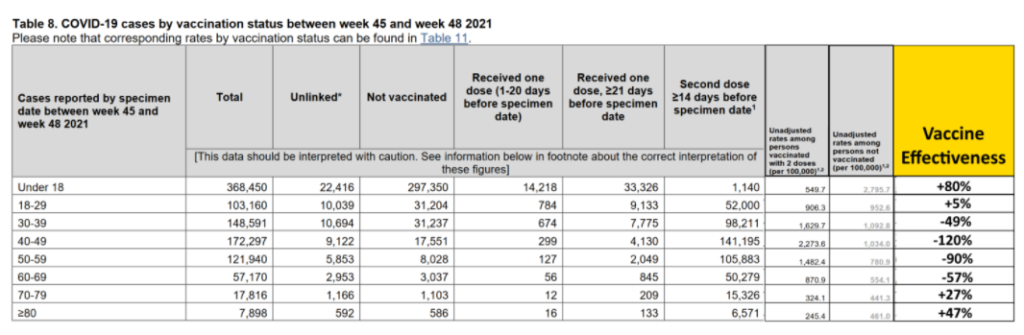
Data provided by the UK’s monitoring system also indicate very low efficacy and demonstrate a constant waning for most age categories:
- U = No. of Cases among the unvaccinated
- V = No. of Cases among the fully vaccinated
- U – V / U = Vaccine Effectiveness
Safety for COMIRNATY (Tozinameran) in the EUDRAVIGILANCE database does look terrible: 700.510 adverse reactions already and 1780 deaths for 2021 following administration of the shots. If one dares comparing with classical vaccines like tetanus or flucelvax that are on the market for many years, one will discover 15,206 adverse reaction reports and 32 deaths for tetanus while the flu vaccine did 280,543 adverse reactions and 1,082 deaths (source VIGIACCESS.ORG from UN).
Without even attempting to go in the causality discussion, it is obvious that something is catastrophically wrong with the covid19 vaccines.
The Pfizer product makes use of two nanoparticles that are NOT suitable for human or animal use, as shown within the datasheets written by the corresponding providers, Echelon Biosciences Inc. and Cayman Chemical respectively:
(Echelon) Hazardous Properties and Cautions: The toxicological and pharmacological properties of this compound are not fully known. For further information see the
MSDS on request. This product is manufactured and shipped only in small quantities, intended for research and development in a laboratory utilizing
prudent procedures for handling chemicals of unknown toxicity, under the supervision of persons technically qualified to evaluate potential risks and authorized to
enforce appropriate health and safety measures. As with all research chemicals, precautions should be taken to avoid unnecessary exposures or risks.
( Cayman) Application of the substance / the mixture
This product is for research use – Not for human or veterinary diagnostic or therapeutic use. It is the
responsibility of the purchaser to determine suitability for other applications
A recent freedom of information act (FOI) request addressed at the state of Japan, revealed serious shortcomings of Pfizer in the context of metabolism of the S-protein and the nanoparticles themselves:
- “Apologize, the S protein from BNT162b2 is expected to undergo proteolysis. From the above, It was considered unnecessary to evaluate the metabolism and excretion of these components again.”
- “Other than the site of administration, it was highest in the liver, followed by the spleen, adrenal glands and ovaries”
“Booster” shots and their repercussions do not appear included in the original trial designs; their safety remains therefore unknown.
According to a recent BMJ article, there are serious allegations that the clinical trial contractor Vantavia manipulated and falsified the trial data (https://www.bmj.com/content/375/bmj.n2635) :
“A regional director who was employed at the research organisation Ventavia Research Group has told the BMJ that the company falsified data, unblinded patients, employed inadequately trained vaccinators, and was slow to follow up on adverse events reported in Pfizer’s pivotal phase III trial. Staff who conducted quality control checks were overwhelmed by the volume of problems they were finding. After repeatedly notifying Ventavia of these problems, the regional director, Brook Jackson, emailed a complaint to the US Food and Drug Administration (FDA). Ventavia fired her later the same day. Jackson has provided TheBMJ with dozens of internal company documents, photos, audio recordings, and emails.”
In between FDA has been ordered by a court to provide all Pfizer vaccine trial data within 7 months instead of granting a moratorium of 75 years.
Immune system
There is controversy regarding the impact of the mRNA injections to the – reprogrammed – immune system. A recent publication explains the negative effects of this reprogramming following mRNA injections and some common by now side effects like herpes zoster: The BNT162b2 mRNA vaccine against SARS-CoV-2 reprograms both adaptive and innate immune responses, Le vaccin à ARNm BNT162b2 contre le SRAS-CoV-2 reprogramme les réponses immunitaires adaptatives et innées, (https://www.medrxiv .org/content/10.1101/2021.05.03.21256520v1).
Pandemic
The impact of the Covid10 pandemic is not at all worrisome, according to a recent Stanford publication (Infection fatality rate of COVID-19 in community-dwelling populations with focus on the persons: An overview, https://www.medrxiv.org/ contenu/10.1101/2021.07.08.21260210v2):
Results Twenty-five seroprevalence surveys representing 14 countries were included. Across all countries, the median IFR in community-dwelling elderly and elderly overall was 2.9% (range 0.2%-6.9%) and 4.9% (range 0.2%-16.8%) without accounting for seroreversion (2.4% and 4.0%, respectively, accounting for 5% monthly seroreversion). Multiple sensitivity analyses yielded similar results. IFR was higher with larger proportions of people >85 years. Younger age strata had low IFR values (median 0.0013%, 0.0088%, 0.021%, 0.042%, 0.14%, and 0.65%, at 0-19, 20-29, 30-39, 40-49, 50-59, and 60-69 years even without accounting for seroreversion).
Conclusions The IFR of COVID-19 in community-dwelling elderly people is lower than previously reported. Very low IFRs were confirmed in the youngest populations.
Early treatment
The question remains, why despite overwhelming evidence that cocktails of generics like hydroxychloroquine, ivermectin, azithromycin, doxycycline and so on, can stop viral replication and accelerate at home recovery, western governments preferred to silence them, suppress the information and outlaw all doctors attempting to honor the Hippocrates oath. A huge number of studies and trials can be found at https://c19early.com/ .
I personally questioned the state’s guidelines and cured myself with the therapeutic protocol of FLCCC, based on ivermectin. Nine months after illness, I presented 1,840 aU/ml antibodies which is not always true for vaccinated people, that only after second shot obtain about 1,000 aU/ml. The BMJ considers a good number the 250 aU/ml.
I understand Merck advising against Ivermectin since that company projected high sales with Molnupiravir (a rather dangerous drug, now forbidden in India) but I find highly UNACCEPTABLE that governments and medical boards do follow and actively support the wishes of the pharmaceutical industry.
These policies are AGAINST citizens and depict a frame of treason when examined against the role that public health organizations should fulfill.
I fear that none of you has dealt with a Covid-19 outpatient and your activities are entirely remote to the primary health-care the way physicians do.
Ethics
Covid-19 vaccines are still experimental:
BNT162b2 is experimental : Estimated Study Completion Date : July 30, 2023 https://clinicaltrials.gov/ct2/show/study/NCT04848584
ARNm-1273 is expérimental: Estimated Study Completion Date : October 27, 2022 https://clinicaltrials.gov/ct2/show/NCT04470427
AstraZeneca is expérimental : Estimated Study Completion Date : August 30, 2022 https://clinicaltrials.gov/ct2/show/NCT05047822
Therefore, the suggestion that these pharmaceutical products of unknown technology are made compulsory does violate several treaties:
UNESCO Universal Declaration on Bioethics and Human Rights (art.6).
Article 6 – Consent 1. Any preventive, diagnostic and therapeutic medical intervention is only to be carried out with the prior, free and informed consent of the person concerned, based on adequate information. The consent should, where appropriate, be express and may be withdrawn by the person concerned at any time and for any reason without disadvantage or prejudice.
UN International Covenant on Civil and Political Rights (art. 7).
Article 7
No one shall be subjected to torture or to cruel, inhuman or degrading treatment or punishment. In particular, no one shall be subjected without his free consent to medical or scientific experimentation.
Universal Declaration of Human Rights
Article 3
Everyone has the right to life, liberty and security of person
Declaration of Helsinki
Informed Consent
25. Participation by individuals capable of giving informed consent as subjects in medical research must be voluntary. Although it may be appropriate to consult family members or community leaders, no individual capable of giving informed consent may be enrolled in a research study unless he or she freely agrees.
In this view, I am unable to find any excuses for your own suggestion about partial obligation to violate entire patient and human rights.
I therefore challenge your advice to the government as beneficial only to the pharmaceutical industry and entirely detrimental to the interests of public health and request its retraction.
Portions of my letter contain material from the excellent report of Canadian doctors, https://www.canadiancovidcarealliance.org/wp-content/uploads/2021/12/The-COVID-19-Inoculations-More-Harm-Than-Good- REV-Dec-16-2021.pdf .
Kind regards
A. Kyriazis
PS: Only two experts found and confirmed in Expertscape with a somewhat poor production the last 10 years.